What it is
- DNA‑based stool test with an at‑home collection kit.

FIT-based national screening programmes like BowelScreen have successfully improved early bowel cancer detection. However, next generation technology can provide additional benefits.

Colosafe® is a home-based, non-invasive bowel cancer screening test that requires no fasting or bowel prep

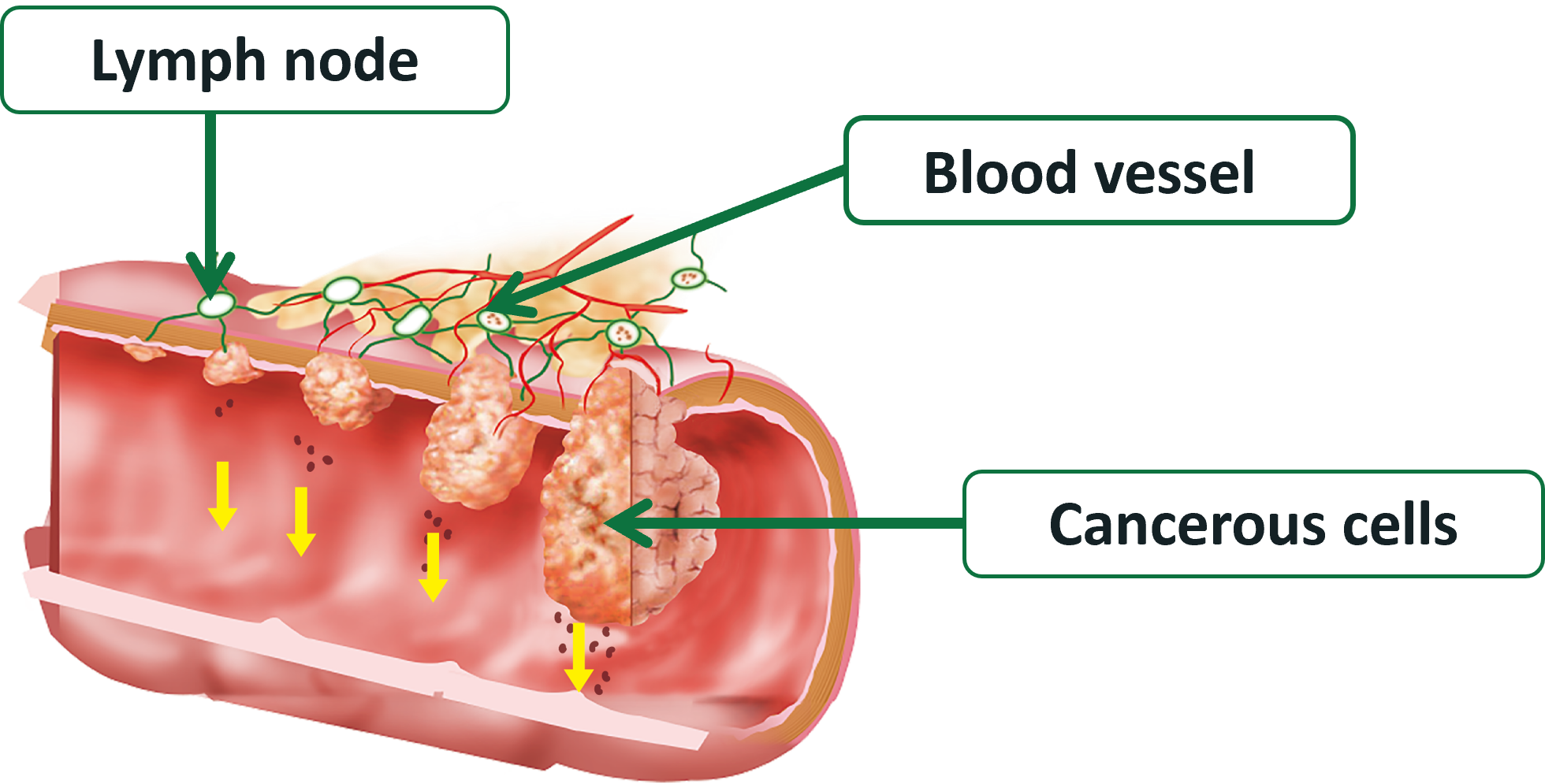
Stool DNA testing detects abnormal changes in exfoliated tumour cells (human SDC2 gene methylation) to help identify early bowel cancer lesions.
The performance of Colosafe® has been well established in international studies and the Colosafe® test has already been used in routine clinical practice with over 1 million patients.
In a multi-centre clinical trial, Colosafe® demonstrated a sensitivity of 83.8% in all stages of bowel cancer, and 87% in Stage I-II CRC with an exceptional specificity of 98% in 1100 participants4.
Adding clinical value when combined with FIT
Colosafe® complements FIT screening by addressing key gaps. Recent data (10,000+ patients aged 45-75, August 2024) demonstrates improved detection of serrated polyps and 99.86% negative predictive value (NPV), reducing both false negatives and colonoscopy burden without compromising specificity5.
Enhanced Sensitivity Profile
Colosafe® demonstrates strong detection capabilities with 86.2% sensitivity for colonoscopy-confirmed CRC compared to 65.5% for FIT (100 ng/ml cut-off), providing clinicians with an additional screening tool for patients who may benefit from heightened sensitivity6.
Adds molecular insight to your decision
Who benefits from Colosafe?
GPs, clinics, pharmacies and healthcare providers can order Colosafe test kits through Eurofins Biomnis and provide them directly to patients.
How to order